Living longer, living well – 25 by 25 in practice in the UK
29th July 2016

29th July 2016
But this may – slowly – be changing. Governments at the World Health Assembly have committed to tackling NCDs, setting themselves a (voluntary) goal to reduce premature deaths by 25% by 2025, known as ’25 by 25’. This has since been echoed in the inclusion of NCDs in the Sustainable Development Goals, which call for a continuation of that trajectory: a 30% reduction by 2030.[1] Sitting behind the 25 by 25 goal are eight supporting targets, including a 30% reduction in salt intake, a 10% reduction in physical inactivity, and (perhaps the most challenging of all) a 0% increase in obesity and diabetes.
But what does a 25% reduction in early deaths really entail? This is the question that the UK’s Richmond Group of Charities set out to answer in Living Longer, Living Well: How we can Achieve the WHO’s 25 by 25 Goals in the UK.[2] It is based on a Policy Review and Modelling Study (PROMISE),[3] extrapolating from existing trends in England to estimate whether ’25 by 25’ can be achieved. Working on the assumption that improvements that have been made in early mortality over the last few decades will continue,[4] the report found that England would not quite reach 25 by 25 – but it would not be far off: 25% fewer premature deaths among women and 22% fewer among men (a total of almost 250,000 deaths from NCDs delayed or averted).
However, the report takes two important further steps. First, it goes beyond the WHO’s 25 by 25 call to look at the potential impact on healthy life expectancy: the number of years that could be lived without disability, including the impact on mental health (particularly depression). And, secondly, it called on a panel of experts to identify a series of interventions that could improve health – four of which have been modelled and their impact on longevity and disability assessed.
The four interventions that are modelled are: reformulating food, increasing tobacco tax, restricting alcohol marketing and fostering physical activity through support from GPs. Although none of these are particularly novel ideas, their potential impact over 10 years, were they to be fully implemented, could be striking. Reformulating food could prevent or delay 27,000 deaths, with 114,000 more years lived without disability. The physical activity intervention could save 11,000 lives and lead to almost 100,000 more healthy years (with a particularly big impact on depression). Even greater reductions in premature death (although this was also the most uncertain and hardest intervention to model, as the researchers acknowledge) could be the impact of restrictions on alcohol marketing.
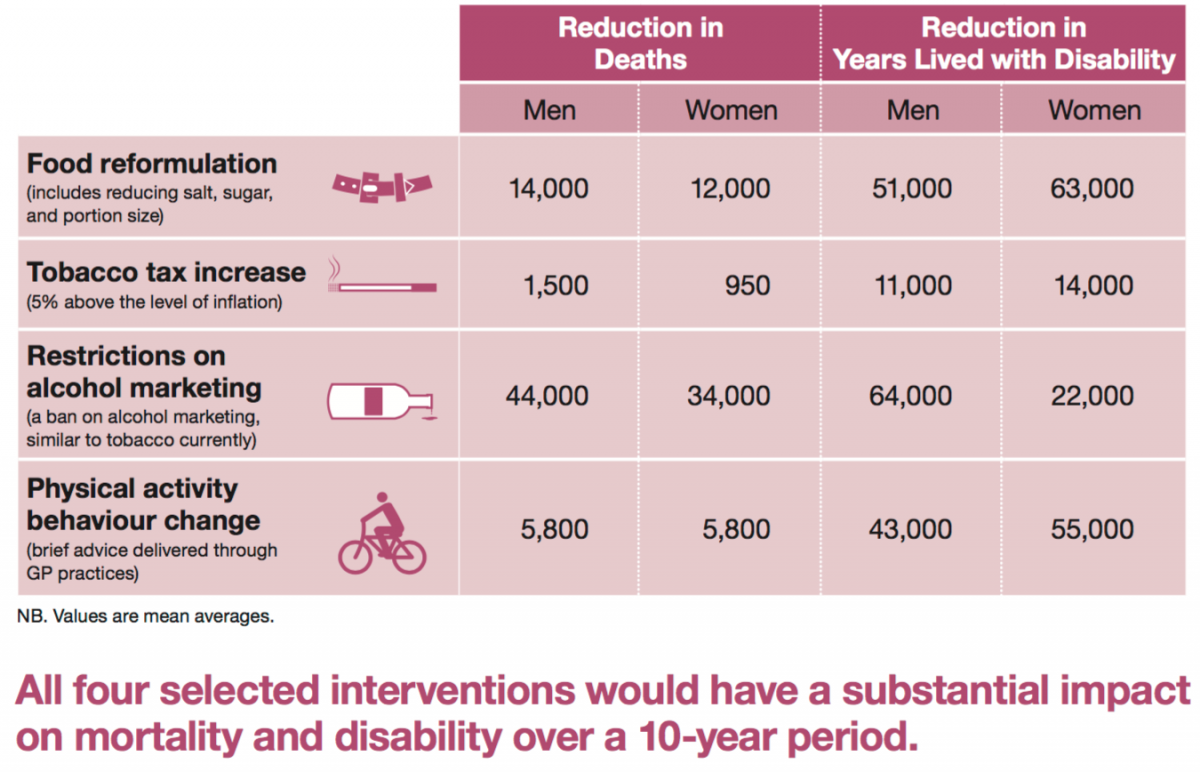
Image: PROMISE modelling demonstrates the impact of 4 interventions on mortality and morbidity in the UK
So – the PROMISE report makes clear that the UK has the opportunity not only to achieve 25 by 25 but also to surpass it, and reduce the number of years lived with physical and mental ill-health. Congratulations to Peter Scarborough, the research team at the British Heart Foundation Centre on Population Approaches for NCD Prevention and the Richmond Group for producing such a thought-provoking report.
The WHO requires reporting by countries on a number of different aspects of NCDs – but is there a reporting versus reality gap? The development of the PROMISE report forms just one of an increasing number of tools and benchmarks that can point the way to real progress. Individual countries are also taking steps nationally, such as Australia’s Health Tracker, featured in a recent NCD Alliance blog.[5] And there are international steps, too. The NCD Alliance has developed a straightforward benchmarking tool for civil society: a core set of indicators that allow in-country progress on NCDs to be assessed.[6] A ‘Scorecard’ on NCDs has also been developed by the Institut de Nutrición de Centro América (INCAP) and C3 Collaborating for Health, surveying experts from government, civil society (NGOs and the private sector) and academia in 23 countries (primarily low- and middle-income countries) to ascertain whether the on-the-ground reality reflects the reporting to the WHO.[7]
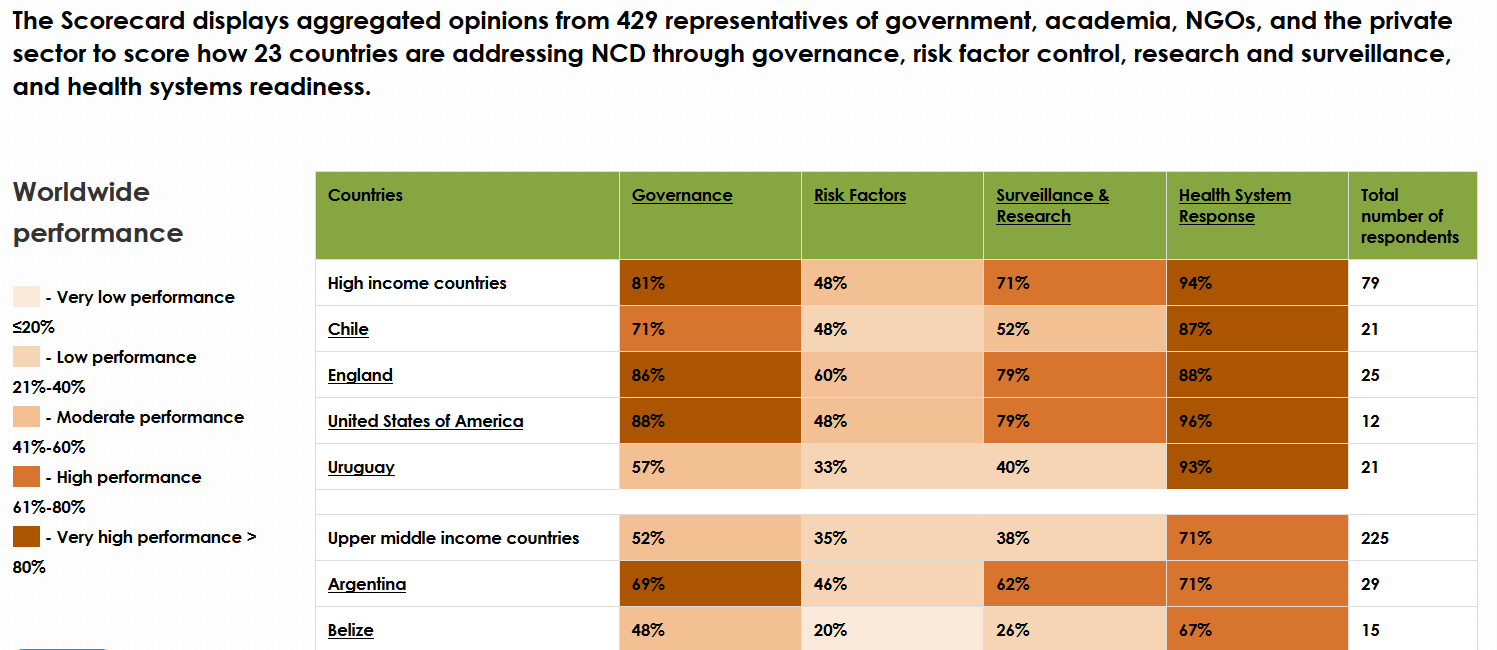
Image: Excerpt of recent findings of the http://www.ncdglobalscorecard.org/
Together, these accountability tools can begin to point the way to real global progress in NCDs – progress that is long overdue.
Katy Cooper is assistant director at C3 Collaborating for Health (@C3health), and has been working in NCD prevention for over a decade. She is an experienced researcher and writer, and works across C3’s portfolio, including workplace and community-based health, and on NCD prevention internationally. In the past she has worked on developing ways to involve businesses in human rights, and she is also both a professional singer and a trustee of Sussex Cricket Foundation.
[1] The SDGs are the successors to the Millennium Development Goals, and are likely to drive the international development agenda for the next 15 years.
[2] Richmond Group, Living Longer, Living Well: How we can Achieve the WHO’s 25 by 25 Goals in the UK (June 2016):
[3] P. Scarborough et al., Translating the World Health Organization 25x25 goals into a United Kingdom Context: The PROMISE Study (full report) (Richmond Group: 2016):
[4] Which is increasingly under question since the launch of the report, as post-Brexit uncertainty may put even greater strain on public-health budgets.
[5] R. Calder et al., ‘Australia's new Health Tracker reveals weak progress towards NCD targets’ (NCD Alliance blog, 4 July 2016):