Health organisations: "Be the change you want to see in the world"

At its simplest level, the job of people wanting to reduce the burden of non-communicable diseases (NCDs) is to “redefine what’s normal”.
We have to make smoke free areas normal. We have to make healthy food routine. We have to make being physically active unremarkable. We have to make non-alcoholic drinks the expected.
Change the default setting
Clearly there are three multi-national industry groups who invest billions of dollars to achieve the opposite – making tobacco smoking, eating junk food and consumption of alcohol as desirable, accessible, socially acceptable and normal as possible.
How do we change a whole society? Where do we start to redefine normal? The obvious answer is in our own backyard. We have a challenge in internal advocacy, before we can meaningfully expect to be taken seriously outside our own walls. It is a challenge because change if not easy. Humans – in general – resist change.
Then
Who could imagine, in 2016, a cancer NGO offering people cigarettes and furnishing ashtrays at meetings? Well, it did happen and it used to be normal. But we changed. Not without pain. Some board members – who were usually smokers – objected.
“But where will we put our ash?”
It won’t be a problem as there will be no smoking in the boardroom.
“But that is outrageous, smoking is legal, and I can smoke everywhere else. People will never accept this. We will be painted as extremists. Mainstream society will abandon us. We will become pariahs. We will lose community support. Our fund raising will fail. We will go broke.”
Smoking causes cancer and we need to set an example.
“But…..”
& Now
Such a conversation seems comical, almost impossible to believe now. But this is mirrored in 2016 when we talk about setting an example on healthy eating, on alcohol and on being physically active.
“How could we run a meeting without offering alcohol? We only want to be seen as hospitable.”
“Why should we meet the cost of offering stand up work stations so people can avoid sitting all day at work?”
“Can we only recruit non-smokers?”
“Cakes, biscuits and sweet treats are just normal parts of catering”
Popular or effective?
Everyone wants to be liked, to be popular. And a way of being so is to conform to, and even reinforce, community norms and customs. By definition, that results in us continuing to do what we always have done.
I tell my own young staff, “I do not hire you to be popular – I hire you to be effective”.
We are agents of change and to change society we must be prepared to make changes internally. And if it is a bit hard to have a no alcohol policy at our organisations’ events – so be it. We are in the change business.
I do not for a moment suggest we must be perfect. I certainly make no such claim for myself. In my private life I might occasionally drink more than 2 standard drinks in a day. And I certainly do not have a perfect diet.
But my job is to promote health. And when doing my job, I, and my organisation, have a responsibility to behave in a manner consistent with the messages we promote.
If a core tenant of our work is to influence society so as to make the “healthy choice the easy choice” then we must demonstrate how to do that. If we cannot - because it is too hard or because we are uncomfortable in breaching community norms - then I’d suggest we are not taking our role seriously. I’d also suggest that in this case we can never win the respect of the communities for whom we work and we have little prospect of success.
Does what I do measure up with what I say? If not – easier to change what I say
Over the past 10 years I have been making this case with people I work with – all around the world.
My observation is that people’s personal behavioural choices, whether it is the amount of alcohol they drink, the type of food they eat, or the extent to which they are physically active, is the single most powerful predictor of their level of support for healthy practice policies.
People do not want to feel like they are being inconsistent. They feel personally vulnerable. This is cognitive dissonance; “inconsistencies among our beliefs, attitudes, knowledge, and/or behaviour can give rise to the uncomfortable feeling of cognitive dissonance”.
Some people can cope with “We need to reduce community alcohol consumption” existing simultaneously with “I plan to share a bottle of wine with my partner tonight over dinner”. Perhaps in the back of their mind they resort to a mistaken belief that “red wine is good for my heart”. The behaviour and the professional belief don’t match.
An organisation that seeks to promote healthy weight and runs a meeting to discuss the learned research and policy to achieve that objective, while serving fried and fatty food with few healthy options is increasingly hard to take seriously.
We should arrange our offices to be healthy. This means standing work stations, healthy catering policies, walking meetings, alcohol free events, all the stuff we encourage in others.
And of course we need to ensure we are not compromised by our funding sources. If we take money from the industries we seek to challenge, again we undermine our own credibility. Think of the effort to manage potential conflict of interest between medical researchers and the pharmaceutical industry. But that is a debate for another day.
If we do not lead by example, I believe we are open to the charge of hypocrisy. And who gives credence to the advice of hypocrites?
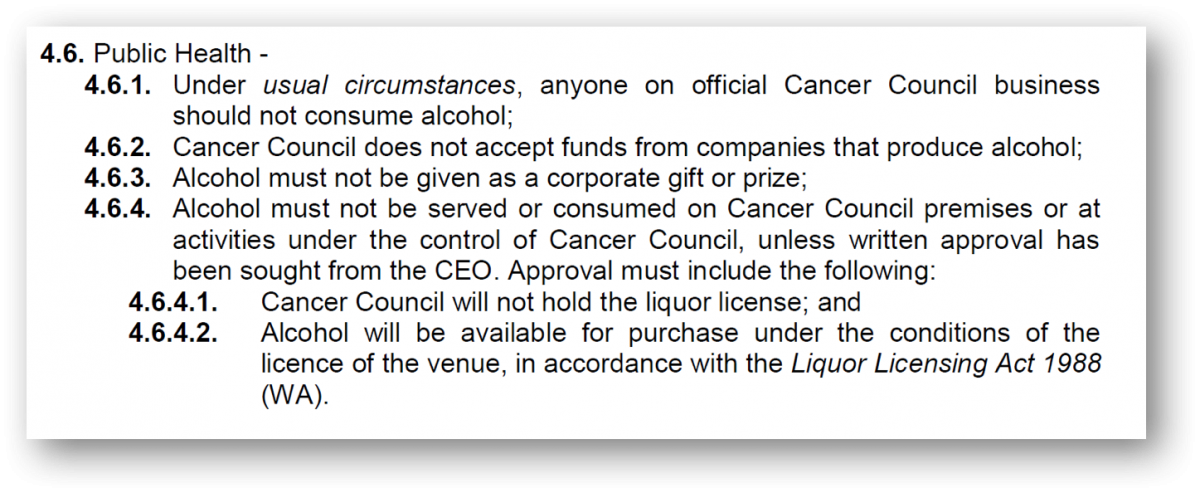
Image: Cancer Council Western Australia's own alcohol policy
About the Author
Terry Slevin (@terryslevin) is Education and Research Director, Cancer Council Western Australia (@CancerCouncilWA) and Adjunct Professor, School of Psychology and Speech Pathology Curtin University. Terry has worked in public health since 1984 and has worked on tobacco control, obesity, alcohol, skin cancer prevention, screening and more. He has published more than 50 papers in the peer reviewed literature and is the editor a book on skin cancer, “Sun, Skin and Health”. He has worked with UICC since 2006.