Our fatal error: Are we looking at the right NCD outcomes?

“Two out of every three deaths are caused by non-communicable diseases.”[1]
In recent years, this statistic has been one of the rallying cries among NCD advocates. It invokes disbelief, disgust, and mobilises people to better address these conditions within the global health agenda. The data from the Global Burden of Disease 2013 visualises this well:
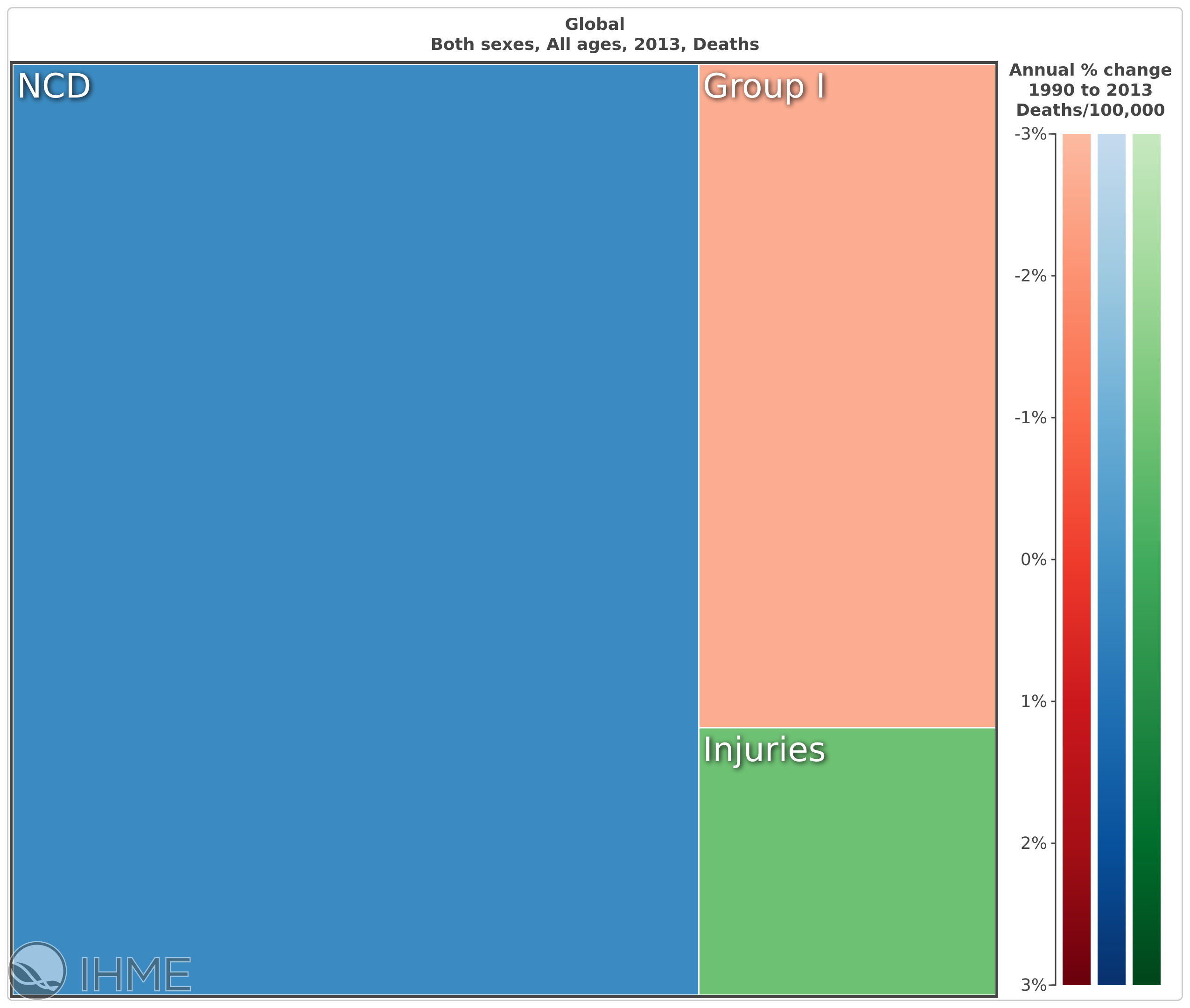
Fig 1: Global Deaths, all ages, 2013: NCDs (blue) 69.75%; Communicable, maternal neonatal and nutritional diseases (red) 21.53%; Injuries (green) 8.72%
On the face of it, this is a compelling argument - we need to better address the issues that cause the most deaths globally.
But when we strip back the details of this statistic, a very different story emerges. In fact, the proportion of NCD deaths rises in tandem with a population’s good health. In Singapore, the healthiest nation on the earth—NCDs account for 77% of all deaths. Japan is even greater at 82%[2].
A healthy society should be dying of NCDs - it’s a reflection that health systems are working, and people are living longer into older life.
The point is that a healthy society should be dying of NCDs - it’s a reflection that health systems are working, and people are living longer into older life. The most common health conditions in older age are non-communicable diseases.
Death is the yard stick by which global health professionals gauge the success of programs and policies.
Whilst the Alma-Ata Declaration and subsequent WHO rhetoric may talk the talk of “health and well-being”, when it comes to health measurement, we assess the exact opposite. Budgets are agreed and interventions are set based on how many deaths can be prevented. More specifically, it is a reduction in deaths in younger life that has received the most attention.
Assessing “year lives lost” better takes this into account. Year lives lost (YLLs) registers not only deaths, but takes into account the age those deaths occur. When we compare deaths to YLLs, the red section of the graphs, which represents issues such as maternal and child health, and communicable diseases like malaria and HIV, become much more prevalent and have dominated the global health narrative, as they stripped young people of their lives.
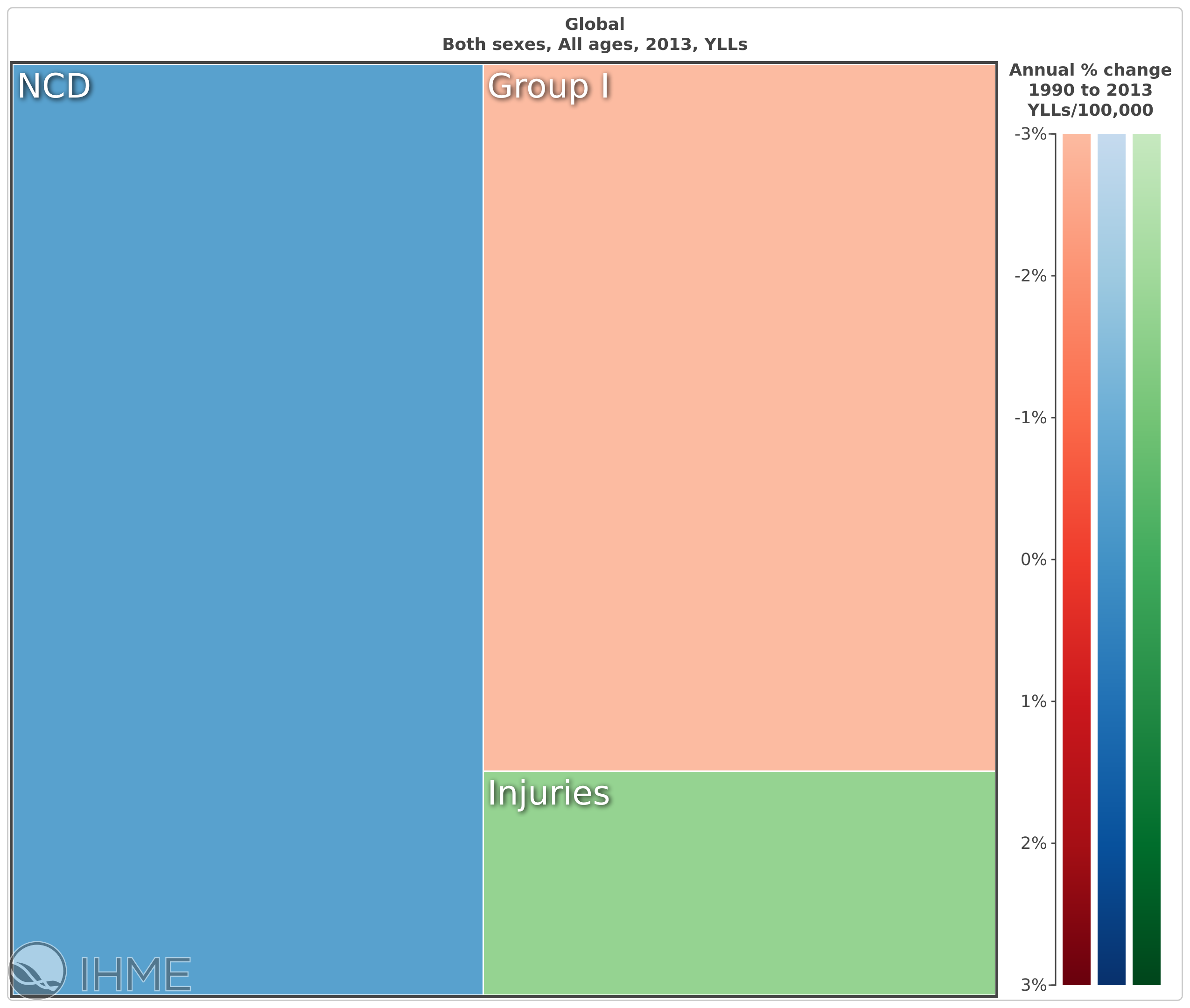
Fig 2: Global year lives lost, all ages. NCDs 47.86%; Communicable, maternal neonatal and nutritional diseases 39.63%; Injuries 12.51%
The success of the health MDGs, which largely focused on issues in this red section, has seen a reduction from around 50% of the total YLL burden in 2010 to 40% in 2013. Yet they still command a significant proportion of the burden and, thus, remain a priority.
It is here where the NCDs are compared in the global health space—pit against communicable diseases in a battle for prioritising on what kills and at what age. By being so tunnel-visioned on death, we have forgotten about how people are affected by NCDs and the disabling consequences of such diseases.
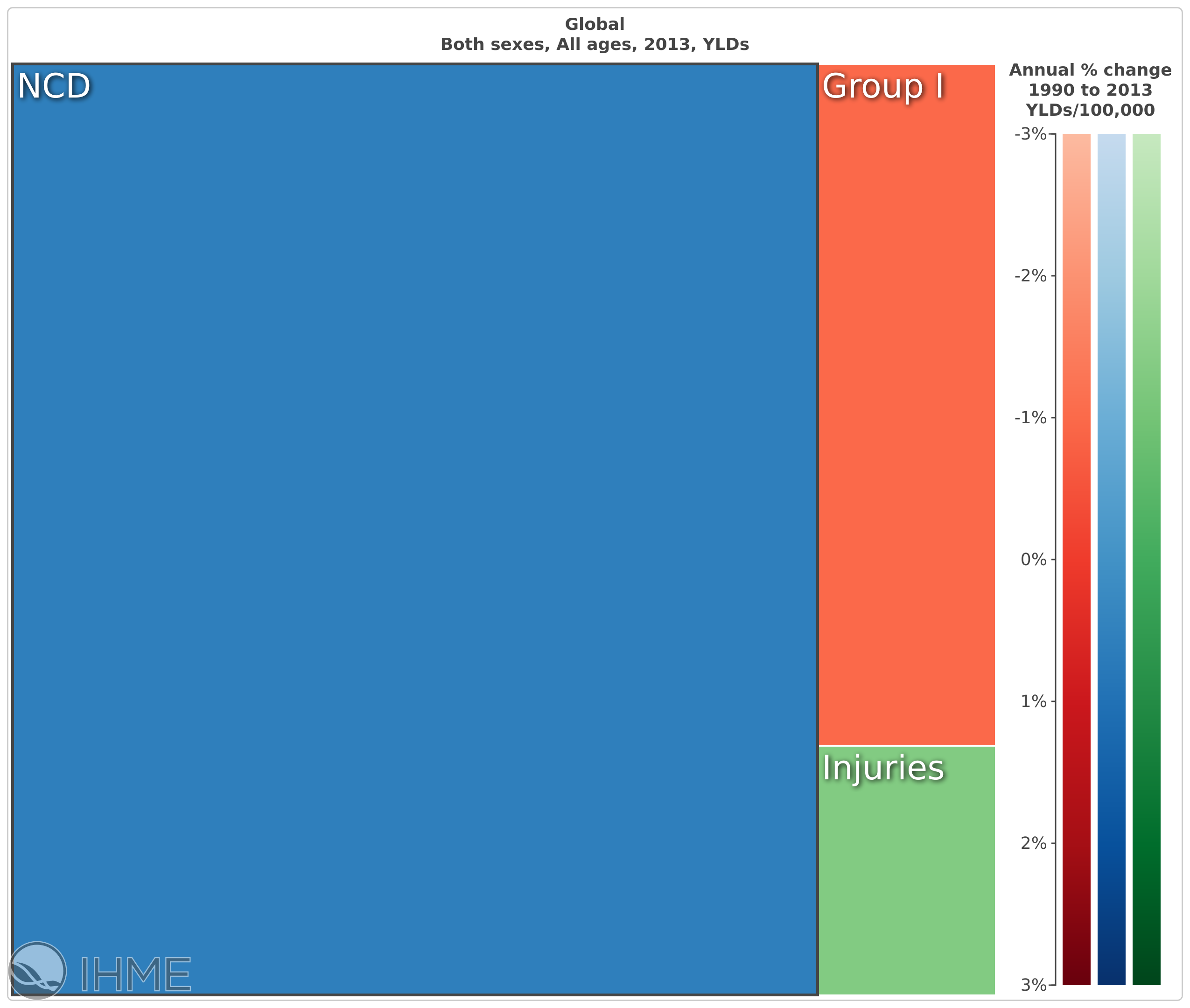
Fig 3: Global years lived with disability, all ages, 2013. NCDs 81.93%; Communicable, maternal neonatal and nutritional diseases 13.25%; Injuries 4.82%
The makeup of these health conditions causing impairments and disability[3] are more varied than those which are the prominent causes of NCD deaths but cause an astounding 82% of all years lived with disability. They include mental health conditions, bone and joint disorders, neurological and other conditions that impact on quality of life and wellbeing across ages.
As a physiotherapist working on rehabilitation programmes around the world, this is the side of NCDs that I most often see. Someone with a lost limb as a result of diabetes, someone too breathless to manage to walk up a flight of stairs due to emphysema, a cancer survivor realising that the fight to survive was just the first step in recovery.
Herein lies the challenge for the NCD community: we have a group of conditions that cannot be truly reflected by death outcomes, yet a measurement system that really only judges success on this morose grading system. In selecting a measure for NCDs we had an opportunity to reshape, to the very core, how we see and measure “health”.
Sadly, that opportunity was not taken and the agreed measure for NCD success reflects ‘premature’ deaths, that is to say deaths amongst people aged between 30 and 70 years old. In order to conform to the standard measure, we have cropped the very population who are most affected by NCDs. By only looking at death, we have ignored the impact that most NCDs have on people, and we have not fully considered the holistic nature of health.
Whilst I have been advocating on this issue for years, this oversight really struck home to me last year when I lost my father to an NCD. Diagnosed with fronto-temporal dementia when he was 58 years old, he lived 12 years past his diagnosis with progressively declining communication capacities, cognitive function, mobility, and personal care. Dying two weeks after his 70th birthday, under our current measurement, this is what an NCD success story looks like. In a world where we know people are living longer, but with more ill health surely our measurement systems need to catch up to the realities of global health in the 21st century. Perhaps that is the different story that NCDs have to tell to get noticed.
We're so tunnel-visioned on death that we've forgotten how NCDs impact life
About the Author:
Antony Duttine (@antduttine) is technical advisor in global health with Handicap International / @HI_UnitedStates, an international NGO focussed on disability in around 60 countries. A registered physiotherapist, he specialised in stroke and cancer rehabilitation in the UK before embarking on work in international development contexts. After living in Namibia and Afghanistan, Antony moved to Washington DC where he now focuses on health policy and advocacy. He has been active within the NCD advocacy community since the UN High Level meeting in 2011. Antony is also a part-time doctorate student at the London School of Hygiene and Tropical Medicine.
[1] NCD Alliance ‘Why NCDs’ https://ncdalliance.org/why-ncds
[2] Data taken from the Global Burden of Disease 2013
[3] Impairments is the term used to reflect issues at the body level relating to function or structures, whereas disability is the much more broad outcome of the interaction of these impairments with environmental and social barriers.
* all data and tables taken from the 2013 Global Burden of Disease report. Visualisations available at http://vizhub.healthdata.org/gbd-compare/
Main image © Erika Pineros / Handicap International Thailand