La santé mentale et le conseil psychosocial doivent être au cœur des programmes humanitaires de prise en charge des MNT

Ce blog explore les résultats d’un programme de MSF de prise en charge des MNT en Syrie avant la guerre. Il souligne l’énorme impact de la guerre et de la condition de réfugié sur la prise en charge et l’autogestion.
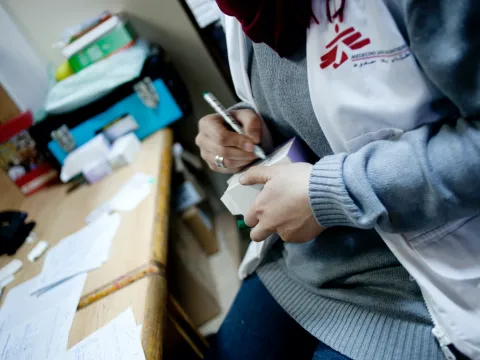
L’épidémie mondiale de maladies physiques non transmissibles (MNT) se produit dans un contexte de crises humanitaires exacerbées. Le programme de prise en charge des MNT de Médecins sans Frontières (MSF) à Irbid (nord de la Jordanie) s’adresse aux réfugiés syriens et à la population jordanienne depuis 2014. L’un des principaux sujets qui ressort d’une évaluation récente du programme est l’énorme impact de la guerre et de la condition de réfugié sur la prise en charge des MNT et l’autogestion des patients.
« Traiter leur MNT ne relève pas des seuls soins médicaux ; ils doivent avoir espoir », explique un médecin qui s’occupe de réfugiés syriens dans le cadre du programme. L’expérience de l’équipe de MSF est venue confirmer le principe selon lequel « il n’y a pas de santé sans santé mentale » : les problèmes psychologiques de leurs patients étaient inextricablement liés à leurs MNT physiques. Impossible de traiter l’un sans l’autre.