Australia's new Health Tracker reveals weak progress towards NCD targets
04th July 2016

04th July 2016
The WHO Global Action Plan for the Prevention and Control of Noncommunicable Disease, 2013-2020 created a contract between the political actors in member states and the citizens those actors represent. This political commitment recognised the primary role of governments in the global challenge to prevent chronic disease.
In Australia, based on the Global Action Plan and facilitated by a health policy think tank, a collaborative network of health NGOs and experts launched a national set of targets and indicators. As the adage goes, with every challenge lies an opportunity; the possibilities to prevent chronic disease are vast. Most premature deaths share common risk factors; tobacco, unhealthy diet, sugar and salt consumption, physical inactivity and harmful use of alcohol.
Many Australian citizens have been holding up their end of the contract. It is routine for individuals with a strong family history of heart disease to visit their family doctor. People living with diabetes regularly check their blood sugar levels. It would seem reasonable, then, for the stewards of the nation’s health system to have regular check-ups too, wouldn’t it? Australia’s Health Tracker is exactly that; a timely assessment of Australian Government efforts to reduce the impact and incidence of chronic disease.
As we stop to check the pulse of chronic disease prevention, has the political commitment translated to action?
In short: no.

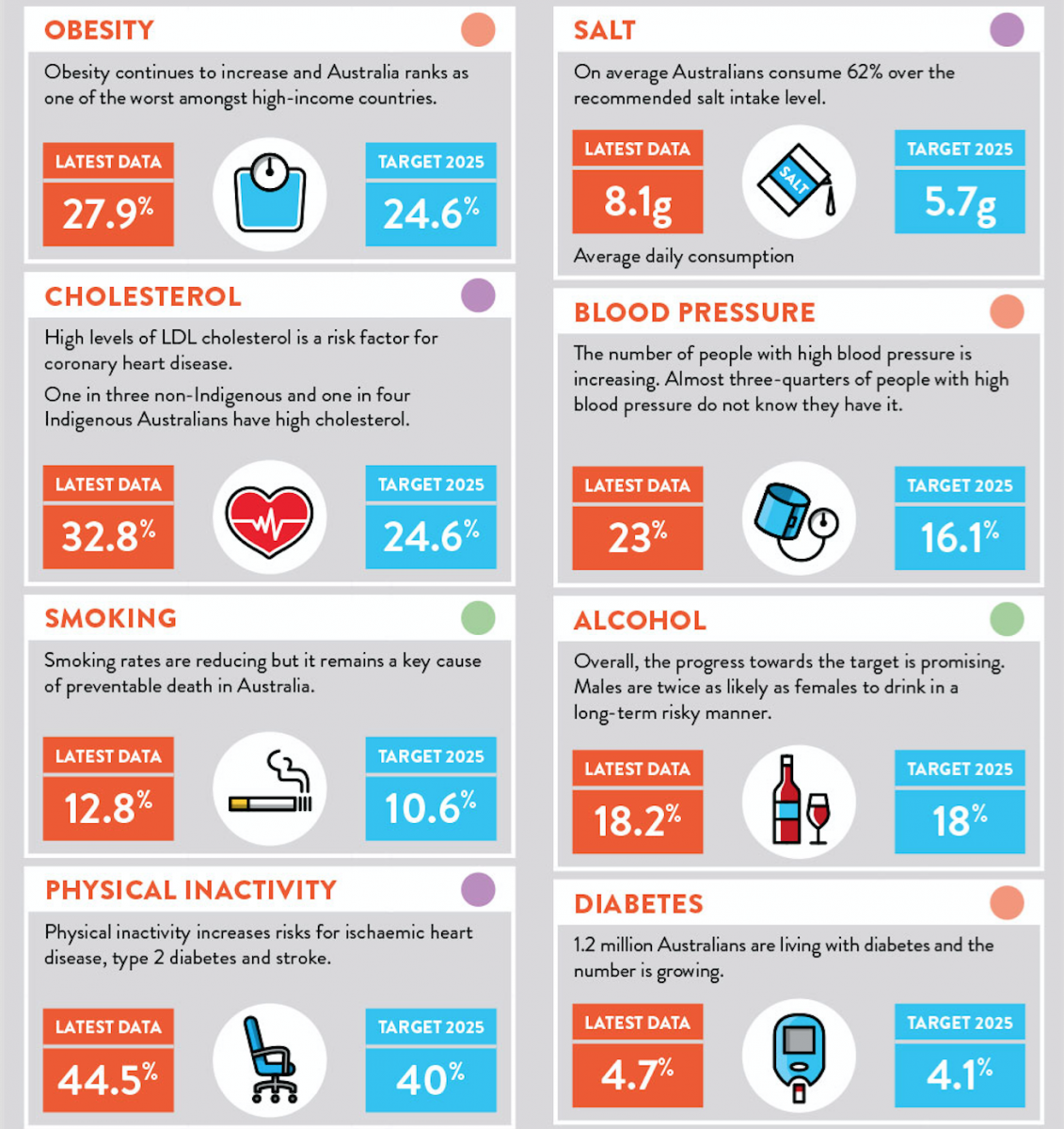
Australia’s Health Tracker, developed by the Australian Health Policy Collaboration (AHPC), provides a snap shot of Australia’s health in terms of preventable chronic disease and conditions, and their most common risk factors. Almost three in four Australian children consume too much sugar, and Australians have among the highest levels of obesity in the world. With the exception of continued tobacco control, the data suggests there is little or no progress being made in preventing and controlling risk factors for chronic disease in Australia. Government concern should be growing further.
Despite renowned public health leadership in tobacco control and road safety, today’s Australia is languishing on its own reputation in preventing and controlling NCDs.
Failure to make progress in relation to harmful alcohol use, poor nutrition and physical inactivity is evidence of a failure to implement cost-effective policy options. Despite many opportunities to invest in the health and wellbeing of Australians, in 2013-2014, government spending on public health (including prevention activities) was a miserly 1.53% of annual health expenditure. Australia is rapidly falling behind comparable health care systems, including Canada (5.9%), Finland (6.1%) and New Zealand (6.4%). Political actors have been unable to translate their commitments to successful policy implementation, and the impact is on the citizens those actors represent.
The failure to invest in chronic disease prevention is a political choice. Share
Aspirational goals are commendable; however, empty promises alone will not ease the growing burden of chronic disease. To achieve a sustained commitment to the substantial challenge of combatting chronic requires a rigorous and independent analysis to encourage and engage political will.
Benchmarking tools can do exactly that.
The Australian network of NGOs and health experts consider that benchmarking tools are leveraged extensively throughout the health care system. For example, to monitor the performance of public hospitals, or to compare health policies of competing political parties in the recent federal election.
Tracking of progress towards the targets and indicators suggests Australia has become complacent and is unlikely to reduce the impact and incidence of chronic disease by 2025.
It is clear that Australian governments now have a chequered history of first agreeing to high-level ‘strategies’ only to retract on specific budgets or agencies required to ensure delivery.
Use of Australia’s Health Tracker as a benchmarking tool, through the leadership and commitment of civil society, can create upward accountability to managers of our health care system; the makers of health policy and sources of finance.
Benchmarking can provide a vehicle for chronic disease actors to strengthen collective advocacy, monitor national progress and create public interest that strengthens the contract between government and society.
The AHPC is not the only organisation sustaining political commitment for action on chronic disease. Civil society status reports have been produced in the Caribbean, South Africa and Brazil. This work has leveraged the NCD Alliance Benchmarking Tool and enabled alliances around the world to influence and monitor NCD policy. Going forward, AHPC plans to produce regular report cards with enhanced granularity on data for specific populations, such as rural and remote areas, low socio-economic or culturally and linguistically diverse demographics.
Such an unflattering assessment is a reminder to all to work harder to fulfil commitments on prevention and control of NCDs.
Tracking progress on policy implementation is not the panacea of prevention. However, it is undoubtedly a constructive and potentially potent step towards better health for all. Australia’s Health Tracker is an unflattering assessment of our nation’s health that reminds governments of their political commitments and opportunities. It is not only the interest of government to honour this social contract. We, Australia’s citizens, must all point to where we want to go, and, what can be done to get there. We can demand and create healthier products, people and places to live and we can aim to ensure the next check-up is a more positive experience for all.
Rosemary Calder AM is Director of the Australian Health Policy Collaboration (@AHPC_VU). She is a respected health and social policy advisor and previously worked as Health Policy Director at the Mitchell Institute and for State and Commonwealth governments. She has experience as a senior public servant for both the Coalition and Labor governments and was head of the Office for the Status of Women, under the Howard Government and Chief of Staff to a former Victorian Minister for Health.
Connor Rochford (@Con_Rochford) is Senior Analyst with Australian Health Policy Collaboration (@AHPC_VU). His academic background is in medicine, public policy and liberal arts, and he recently worked with McKinsey and Company. He is driven by a desire for global health; a world of affordable and accessible health care. Connor is particularly passionate about responding to the impact of population change at the interface of health, social and economic policy. His research interest surrounds the policy implications for health and long term care.
Rob Moodie (@ARobM) is currently Professor of Public Health at the College of Medicine, University of Malawi, and Professor of Public Health at the University of Melbourne’s School of Population and Global Health (MSPGH). He was CEO of VicHealth from 1998-2007, the world’s first health promotion foundation based on a dedicated tobacco tax. From 2008-2011 he chaired the National Preventative Health Taskforce in Australia and, in addition to teaching, advises the World Health Organization in the areas of Non Communicable Diseases and Health Promotion.
