
Joining from Women Deliver? See our list of resources.
Fast Facts
- NCDs kill two out of every three women. A gender lens to NCDs is needed to understand the NCD burden among women so that inequalities are addressed.
- Women face limited access to quality health services and are often more exposed to NCDs and their risk factors due to gender norms, resulting inequality, and a range of related economic and social factors, especially in low-resource settings.
- Integrating maternal and child health with NCD care represents an opportunity to reduce preventable maternal deaths and improve the health of women.
- Some industries selling harmful products are increasingly targeting women through aggressive marketing tactics. From the formula milk industry to other sin industries like tobacco and alcohol, women are seen as a business opportunity at the expense of their health.
- Universal Health Coverage (UHC) has the capacity to reduce many of the disadvantages that women experience in relation to NCDs when designed and implemented from a gender perspective.
Gender inequality and NCDs
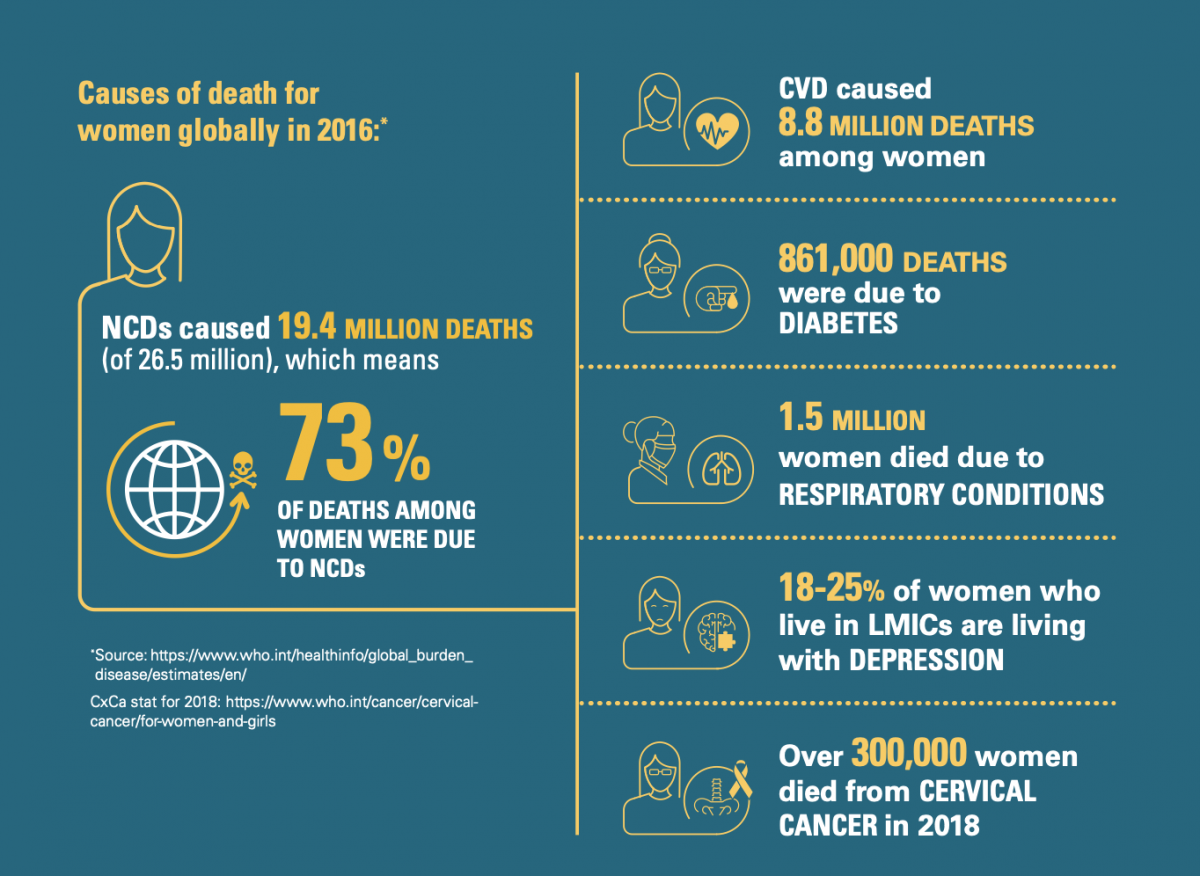
Two out of every three women die from an NCD, accounting for up to 19 million deaths every year, nearly half of them being caused by cardiovascular diseases (CVD) alone. Gender norms, resulting inequalities and other intersecting determinants cause women and girls to experience a number of disadvantages that make them particularly vulnerable to NCDs, especially in low- and middle-income countries (LMICs).
This is why taking a gender lens is crucial to ensure an equitable response to NCDs and drive forward the sustainable development agenda.
Around the world, women face significant barriers to access of timely, adequate, or affordable health screening and care. This often results in poor health outcomes and high rates of deaths – and particularly in low-resource settings.
In these settings, families may prioritise the healthcare needs of children and men over those of women, who are usually the sole caregivers in the household. Travel time and cost may also make women less likely to access health services, prioritising instead their household responsibilities.
Women may also have limited financial decision-making power in the household – or decision-making power in general – which significantly impedes on their ability to manage their health. In addition, many female-specific conditions – such as breast and cervical cancer (killing over 300,000 women every year) – carry a stigma which acts as a barrier to detection and treatment. [1]
Women with low socio-economic status are often at higher exposure to NCD risk factors due to gender norms. Proof of this is that, in many LMICs, women present lower levels of physical activity in relation to men as a result of social and cultural customs related to gender and mobility [2]. In addition, women and girls are more likely to receive less education than men, thus limiting their capacity to inform and protect themselves against other risk factors for NCDs, including unhealthy diets, air pollution, tobacco and alcohol use.
Maternal and child health: a case for integration with NCDs
In many countries, there is a foundation of strong maternal and child health services that was driven by the Millennium Development Goals (MDGs), which ran from 2000 to 2015. However, declines in maternal death rates have since stalled. It's projected that more than 1 million women will die by 2030, and nearly all of them in LMICs, if we are to stick to the current maternal death rate of 223 maternal deaths per 100 000 live births.
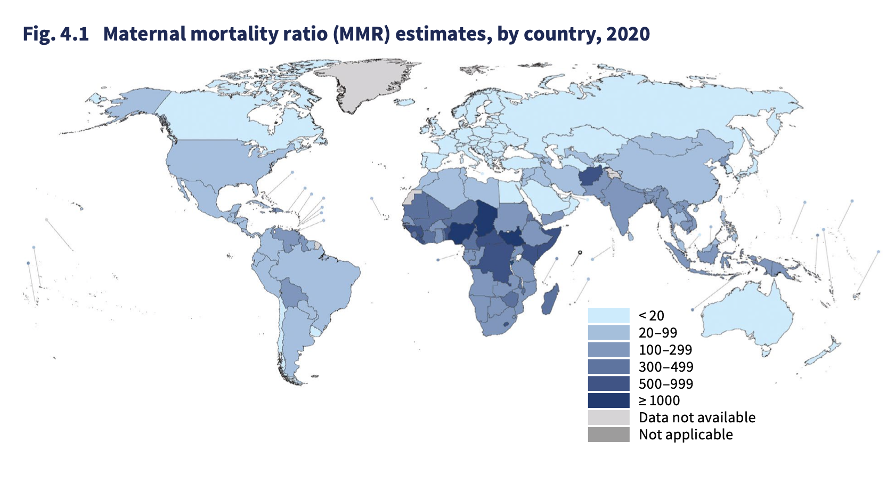
Trends in maternal mortality 2000 to 2020, WHO et al, 2023
Progress made is at risk of being rolled back as a result of untreated NCDs related to maternity like hypertensive pregnancy disorders, which account for 10% to 15% of maternal deaths in LMICs. [3] Beyond that, the occurrence of other NCDs such as diabetes or cardiovascular disease (CVD) significantly affects the health of pregnant women and their unborn children.
Nearly all deaths due to complications of pregnancy and childbirth can be prevented. There is a need to integrate the prevention, screening, and treatment of NCDs into existing maternal, child, and adolescent health programmes, as recognised in the Global Strategy for Women’s, Children’s and Adolescents’ Health (2016-2030).
Integration would also help to prevent inter-generational transmission, as children born to mothers with uncontrolled NCDs risk developing poor health later in life. While the diagnosis of pregnancy-related NCDs like gestational diabetes mellitus (GDM) or preeclampsia (which presents as high blood pressure) can help to identify women who are at an increased lifetime risk of other underlying chronic diseases. [4]
Unhealthy industries target women
Some industries selling harmful products see women as a business opportunity. This is the case of the baby food industry, which is known for using aggressive marketing strategies to inappropriately market formula milk as a healthy substitute for mothers’ milk, or even as necessary for children.
Breastfeeding has numerous health benefits since it protects children from child malnutrition and obesity while reducing women’s risk of diabetes, obesity and some forms of cancer. However, as breastfeeding rates worldwide have increased very little in the past two decades, sales of formula milk have more than doubled in roughly the same time.
So-called sin industries like the tobacco industry and the alcohol industry are also seeking to expand their market share at the expense of women’s health. After narrowing the consumption gap between men and women in many higher-income countries, Big Tobacco is now targeting girls and young women in LMICs, where female smoking is much less prevalent. While tobacco use remains lower among women than men around the world, girls are recording higher consumption levels than adult women and boys in many countries. [5]
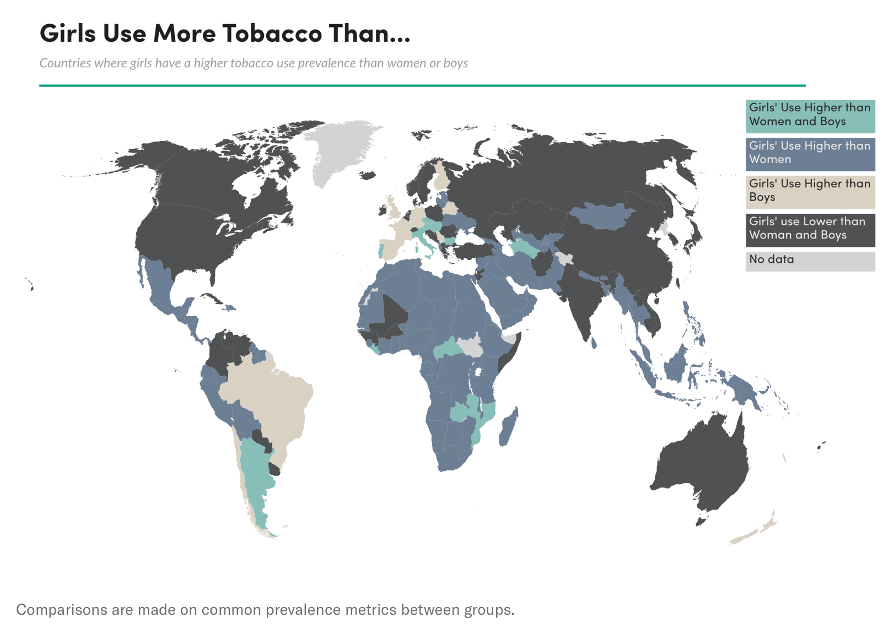
Tobacco Atlas, 2020
Following in the footsteps of the tobacco industry, Big Alcohol is shifting its marketing efforts towards women, who have historically drank much less than men in most countries. As a result, alcohol use among women has increased, especially among young women. [6]
Gender lens to Universal Health Coverage
Many of the disadvantages in access to healthcare and the resulting burden of NCDs and their risk factors stem from the fact that girls and women are hit hardest by poverty. This is concerning given that 85% of premature deaths from NCDs (i.e. between the ages of 30 and 70) occur in LMICs.
However, social factors like education, race, ethnicity, age, disability, power and autonomy also prevent women from being able to protect themselves from NCDS and access quality healthcare.
Universal Health Coverage (UHC) has the potential to reduce health inequalities faced by women, but health systems and policies need to be designed and implemented in a way that is affordable, accessible to them, and informed by their involvement in a particular setting.
Considering the financial barriers to health that women face, the implementation of a system of UHC would benefit most women, and particularly those in LMICs, thus contributing to their economic potential and capacity to lead a healthy life.
UHC packages should include high-impact primary healthcare in a one-stop shop. These include sexual and reproductive health services, pre- and antenatal care, breast and cervical cancer screening, and testing for other infections like HIV and TB.
A gender-responsive UHC will also ensure that no woman and girl is left behind, and that non-financial barriers to accessing healthcare are also addressed.
These include coverage of services that are culturally sensitive and women-friendly, utilising differentiated care models that reach the most vulnerable or marginalised.
Poor design of services can perpetuate or exacerbate structural inequalities. Evidence of this may be found in countries where gender disparities in access to care have arisen despite publicly funded healthcare systems being in place. In the UK, for example, women were found to be 13% less likely than men of the same age to receive a prescription for the two most important drugs in heart failure management within three months of diagnosis. [7]
Universal Health Coverage policies that address the gender determinants of health have the potential to turn the tide on women’s health, and will help us to achieve gender-related sustainable development goals.
Page last updated: 8/3/2023